
You’re 32. You eat reasonably well. You wash your face. So why does that same spot on your jawline keep coming back? Adult acne affects up to 50% of women in their 20s and persists into the 40s for many. The frustrating truth: what worked for teenage acne often makes adult acne worse. This guide breaks down what’s actually happening beneath your skin, why your “normal” lab values may not be optimal, and what dermatology-informed care actually looks like in 2026.
How Acne Actually Forms
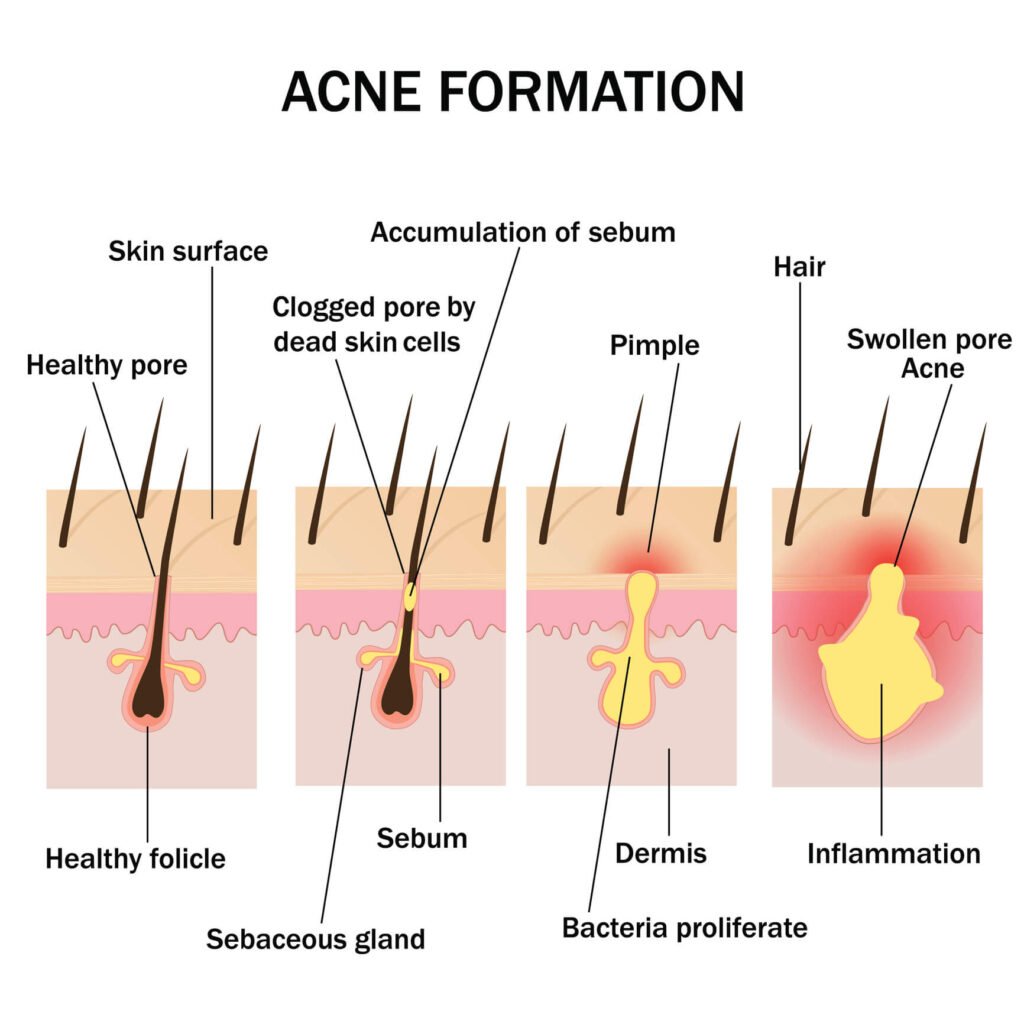
Acne develops through four interconnected mechanisms. Understanding each helps explain why some treatments work and others don’t, and why the same product can clear one person’s skin while making another’s worse.
First, your sebaceous glands produce excess oil (sebum) — often driven by hormones, stress, or genetics. Second, dead skin cells fail to shed properly and accumulate inside the pore. Third, this trapped mixture creates an ideal environment for Cutibacterium acnes bacteria to multiply. Fourth, your immune system responds with inflammation — the redness, swelling, and pain you actually see.
Each of these four steps is a potential intervention point. The diagram below shows how a healthy pore progresses through these stages into visible acne.
The Four Faces of Adult Acne
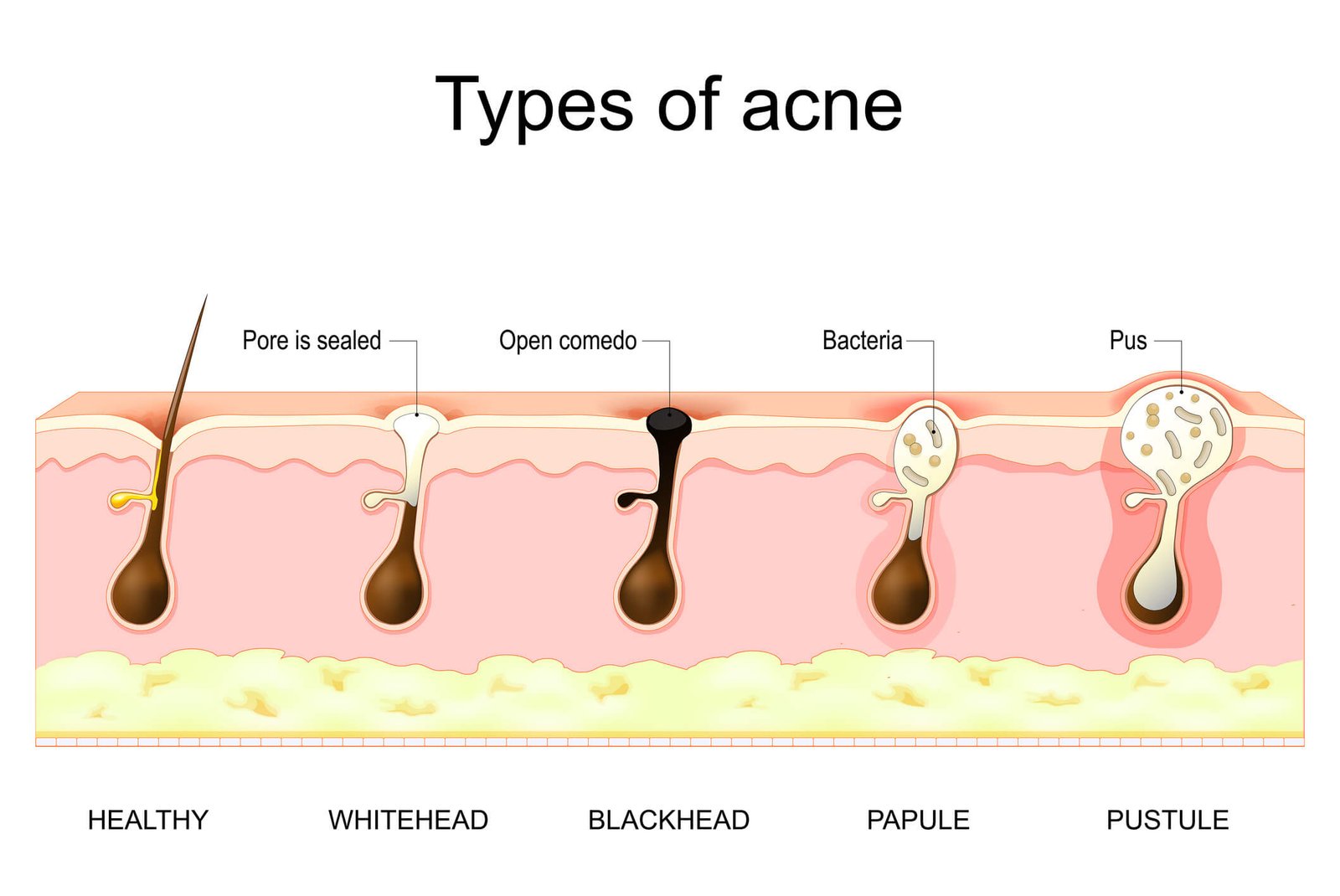
Not all acne is the same, and treating every breakout the same way is one reason many people stay frustrated with their results. Adult acne typically falls into four distinct patterns, and identifying yours is the first step toward effective treatment.
Comedonal Acne (Whiteheads & Blackheads)
Comedonal acne shows up as small bumps without redness — the classic blackheads and whiteheads, usually on the forehead, nose, and chin. It’s caused by clogged pores rather than infection or inflammation. This type often responds well to over-the-counter retinoids and salicylic acid, though patience is essential since visible improvement typically takes 8 to 12 weeks.
Inflammatory Papules (Red, Tender Bumps)
Inflammatory papules are the red, tender bumps without a visible white head. They tend to appear on the cheeks and around the mouth, and they signal that bacteria and immune response are involved. Treatment usually combines a retinoid with a topical antibiotic or benzoyl peroxide, though the two should never be applied at the same time.
Cystic & Nodular Acne (Deep, Painful Lesions)
Cystic and nodular acne is the most painful and stubborn type. These deep, swollen lesions form along the jawline, chin, and neck, and they often leave scars even after they heal. Topical treatments alone rarely work for this pattern. If you’re dealing with cystic acne, prescription medications like oral isotretinoin or hormonal therapy are usually the most effective path forward.
Hormonal Acne (Cycle-Related Breakouts)
Hormonal acne follows your menstrual cycle, flaring on the lower face — chin and jawline — in the week before your period. It can overlap with any of the other types and is especially common in women in their late 20s and 30s. Hormonal acne often persists despite a good skincare routine because the root cause is internal, not topical.
Not sure which type you’re dealing with? Your acne pattern determines everything about what works.
Join the Waitlist4 Myths That Keep Your Skin Breaking Out
Misinformation about acne is everywhere, and following the wrong advice can actually make breakouts worse. Let’s clear up the most common myths that may be sabotaging your skin.
Chocolate & Acne
❌ MYTH
Chocolate causes acne.
✓ TRUTH
Chocolate itself isn’t the culprit. High-glycemic foods (sugary drinks, white bread) and skim milk are the real triggers in some studies. Track your patterns over weeks instead of cutting foods you love.
Face Scrubbing
❌ MYTH
Scrub your face hard to clear acne.
✓ TRUTH
Aggressive scrubbing damages your skin barrier and triggers more breakouts. Acne isn’t caused by dirty skin. Cleanse twice daily with a gentle, non-foaming cleanser.
Moisturizer & Oily Skin
❌ MYTH
Skip moisturizer if you have oily skin.
✓ TRUTH
Skipping moisturizer makes skin produce more oil, not less. Use a non-comedogenic, oil-free moisturizer with hyaluronic acid or niacinamide — especially when using retinoids or benzoyl peroxide.
Tanning & Acne
❌ MYTH
A tan clears acne.
✓ TRUTH
Tanning only masks redness temporarily. UV exposure triggers more breakouts, accelerates aging, and damages your skin long-term. Daily SPF 30+ is non-negotiable, even with breakouts.
The Diet, Hormones & Bloodwork Connection
If you’ve been treating your skin topically for years with no results, the answer often lies deeper. Two patterns matter most for adult acne, and both are commonly missed by general skincare advice.
High-glycemic foods and dairy spike insulin and IGF-1, which directly drive sebum production. Sugary drinks, white bread, sweets, and especially skim milk are the most studied culprits. The Mediterranean diet pattern, by contrast, has clinical evidence for reducing breakout frequency — likely through lower glycemic load and higher anti-inflammatory omega-3 intake.
Persistent jawline acne, irregular cycles, and unwanted hair growth often signal hormonal imbalances like PCOS. These signs require specific medical evaluation — not just topical creams. If your acne flares predictably with your cycle, hormones are part of your equation.
“Normal” is not “Optimal” for your skin.
Most patients are told their bloodwork is “normal” by general practitioners. But in clinical dermatology, being within the laboratory reference range doesn’t mean your levels are optimal for skin repair. Your ferritin or vitamin D might be technically “normal” yet still insufficient to support the cell turnover needed to clear acne and heal scars. Skin needs a higher bar.
“In ten years of dermatology practice, the single most common pattern I see in adult acne patients is this: they’re treating yesterday’s skin with yesterday’s products. The teenager who used harsh foaming washes and 10% benzoyl peroxide is now a 32-year-old with a compromised barrier — and the same routine is the reason her acne won’t clear. Adult skin needs gentler chemistry, deeper investigation, and patience measured in months, not days.”
⚠ When to See a Dermatologist
Some signs warrant prompt medical evaluation
If any of the following describe your situation, don’t wait — book a dermatology consultation:
- Deep, painful nodules or cysts that last more than a few weeks
- Scars or permanent dark marks beginning to form
- Sudden severe acne with no prior history
- Hormonal signs: irregular periods, hirsutism, or hair thinning
- No improvement after 3+ months of consistent over-the-counter treatment
- Significant emotional distress, anxiety, or social withdrawal
Early intervention prevents permanent scarring and saves months of trial and error.
What Actually Works: Treatment Categories
Modern acne treatment goes far beyond benzoyl peroxide and “wait it out.” Today’s evidence-based options span five distinct categories, and the right approach depends on your acne type, severity, and overall skin profile. Most effective treatment plans combine two or three of these.
Topical Retinoids
Topical retinoids are the foundation of nearly every effective acne routine. Adapalene (now available over-the-counter), tretinoin, and trifarotene work by normalizing how skin cells shed inside the pore — preventing the microcomedones that become future breakouts. Expect 8 to 12 weeks before visible results, and pair with a non-comedogenic moisturizer to manage initial dryness.
Benzoyl Peroxide
Benzoyl peroxide kills C. acnes bacteria within the pore and reduces inflammation. It’s most effective for inflammatory papules and pustules, and unlike antibiotics, bacteria don’t develop resistance to it. Start with 2.5% — higher concentrations cause more irritation without significantly better results. Never apply at the same time as retinoids; alternate morning and evening instead.
Salicylic & Azelaic Acid
Salicylic acid penetrates oil to unclog pores from within, making it ideal for blackheads and whiteheads. Azelaic acid is a gentler alternative that also fades post-acne dark spots — particularly valuable for sensitive skin or melanin-rich complexions where post-inflammatory hyperpigmentation is a concern. Both are well-tolerated during pregnancy when retinoids are off-limits.
Oral Medications
For moderate-to-severe or stubborn acne, prescription oral options change the equation entirely. Short-course antibiotics (doxycycline, minocycline) reduce inflammation, hormonal therapies (spironolactone, combined oral contraceptives) target the root cause in women with hormonal acne, and isotretinoin remains the most effective treatment for severe cystic and scarring acne — often producing long-term remission.
Procedural & Lifestyle Support
Chemical peels, light-based therapies, and microneedling can accelerate clearing and address acne scars when topical care alone isn’t enough. Equally important are the daily habits — consistent sleep, stress management, and a low-glycemic diet — that determine whether your treatment plan reaches its full potential. Skincare doesn’t work in isolation from the rest of your life.
Which combination is right for you depends entirely on your acne type, severity, age, hormonal status, current medications, and skin sensitivity. There’s no one-size-fits-all protocol.
Stop guessing. Start treating the skin you actually have.
A dermatologist-informed read on your acne type, triggers, and the exact routine your skin needs.
Reserve My SpotFrequently Asked Questions
How long does it take for acne treatment to actually work? +
Most evidence-based treatments require 8 to 12 weeks of consistent use before noticeable improvement, and many require 3 to 6 months for full results. Stopping early is the most common reason for “treatment failure.” Patience and consistency matter more than constantly switching products.
Is adult acne different from teenage acne? +
Yes, significantly. Adult acne tends to be more inflammatory and hormonal, concentrated on the lower face — chin, jawline, and neck. It often coexists with skin sensitivity, dryness, and early signs of aging, which makes treatment trickier. Strong products that worked at 16 often damage the skin barrier at 35.
Can I use retinoids and benzoyl peroxide together? +
Not at the same time — benzoyl peroxide can deactivate certain retinoids like tretinoin, and the combination is highly irritating. The standard approach is to alternate: benzoyl peroxide in the morning, retinoid at night. Adapalene is more stable and can be used alongside benzoyl peroxide if needed.
Should I see a dermatologist or try over-the-counter products first? +
If you have any of the red flags listed earlier — deep cysts, scarring, sudden severe acne, or hormonal signs — see a specialist promptly. Otherwise, a personalized skin assessment can help you identify your acne type and build an effective OTC routine before considering prescription options. For a full overview of evidence-based treatment options, the AAD acne guidelines are a reliable reference.
Does diet really affect acne? +
For some people, yes — measurably. The strongest evidence links high-glycemic foods (sugary drinks, white bread, sweets) and skim milk to increased breakouts in susceptible individuals. Chocolate itself is neutral; the sugar in chocolate may be the issue. The Mediterranean diet pattern has clinical evidence for reducing acne severity. Track your patterns over 6 to 8 weeks before drawing conclusions.
Reviewed by a practicing dermatologist with 10+ years of clinical experience. All content checked against current AAD and EADV guidelines before publication. About our editorial standards →
Medical Disclaimer: This content is for informational and educational purposes only and does not constitute medical advice, diagnosis, treatment, or a substitute for professional dermatological care. If you have a persistent, changing, or concerning skin condition, please consult a dermatologist.


